
When a person dealing with trauma says to their therapist, “I can’t talk about it,” this is not a dead end. It’s not blocking therapy.
Far from it. It is the beginning of the work; it shows exactly where it needs to start.
“I can’t talk about it” is not resistance. It is information. It tells us that one or more barriers are in place. These barriers need to be identified, brought into the open, and presented to the client for consideration.
In short, “I can’t talk about it” contains enough information to guide the next phase of therapy, if its internal logic is made explicit.
Discovering Disclosure Barriers Is Therapy Gold
Finding these barriers is not a preliminary step. It is a vital part of the therapy.
The position of “I can’t talk about it” is itself a Stuck Point – one of those rigid, distressing thoughts and beliefs that feel impossible to move beyond.
Stuck points are often the mind’s default response to unprocessed trauma. They are not random. They are structured attempts to make sense of overwhelming experience.
What Sits Behind “I Can’t Talk About It?”
In therapy, it is often enough for now to talk about why you can’t talk about it. That is not avoidance. That is a large part of the work.
Like a form of emotional echo-location, we can begin to map the terrain indirectly.
By exploring the barriers and ‘exemptions’, we begin to understand:
- The shape of the trauma
- Its weight
- Its personal meaning
We may not be talking about the event itself yet, but we are getting very close to it.
Stuck Points Rarely Come Alone
Stuck points tend to multiply across time. The original traumas often give rise to unhelpful beliefs that harden into stuck points.
By exploring a person’s:
- View of the past
- View of the trauma(s)
- View of the time between trauma and now
- Experience of the present
- Expectations of the future
we can build a Timeline of Stuck Points, as shown in the diagram below.
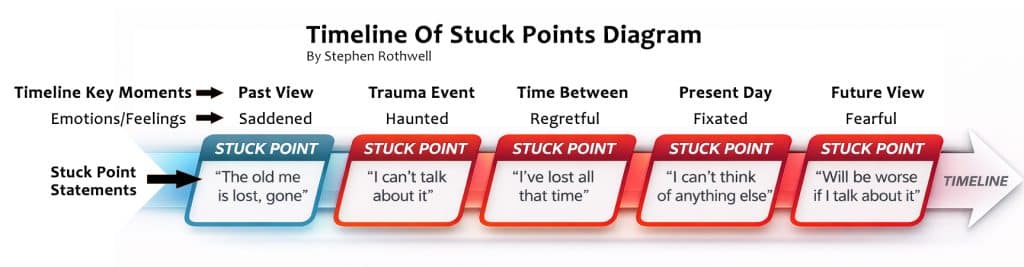
Note how for each Timeline Key Moment, there are emotions/feelings attached.
Then, in each of the red boxes there are Stuck Point Statements.
Seeing the System Can Change Everything
You see now how we have a lot more information to work with.
We now know a lot more fixed beliefs and mental loops: Stuck Point Statements. What emerges is not a single belief, but a network of fixed positions, and how the person feels about them.
For many people, this is the first time they see the full picture. Thoughts that once felt chaotic and intrusive are now named, organised and contained.
Damaging thoughts that came into consciousness; caused harm and faded away, only to loop around repeatedly, now become known, visible and accounted for.
What once swirled unpredictably now has coherence, shape and boundaries.
That alone has therapeutic value.
When people see how many stuck points they are carrying, something often shifts.
There is often a moment of recognition, even shock. The realisation comes,
“All this has been running my thinking.”
In many cases, the person has already begun opening up, without realising it.
By describing their beliefs across time, they have revealed:
- How the trauma shaped their identity
- How it influenced their interpretations
- How it continues to operate
From here, some stuck points can begin to loosen.
For example:
“The old me is gone” may soften when examined more closely. It may be that the past is being viewed through a rose-coloured nostalgic lens, and that in truth, there were significant life difficulties before the main trauma event(s) occurred.
This does not dismantle the belief entirely. But it creates a small opening.
And sometimes, that is enough.
From Mapping to Movement
Through a combination of:
- Recognising the cumulative weight of multiple stuck points
- Gently re-examining less rigid beliefs
The conversation can begin to shift.
The trauma, once avoided, sometimes becomes:
- Something that can be approached
- Something that has edges
- Something that can be worked with
From there, deeper phases of therapy may become possible.
But It Is Not Always That Straightforward
In many cases, the barriers are more entrenched.
This is where a deeper understanding becomes necessary.
‘I Can’t Talk About It’ and Stacked Disclosure Barriers
“I can’t talk about it” stuck points do not always operate in isolation.
They can combine. They can reinforce each other.
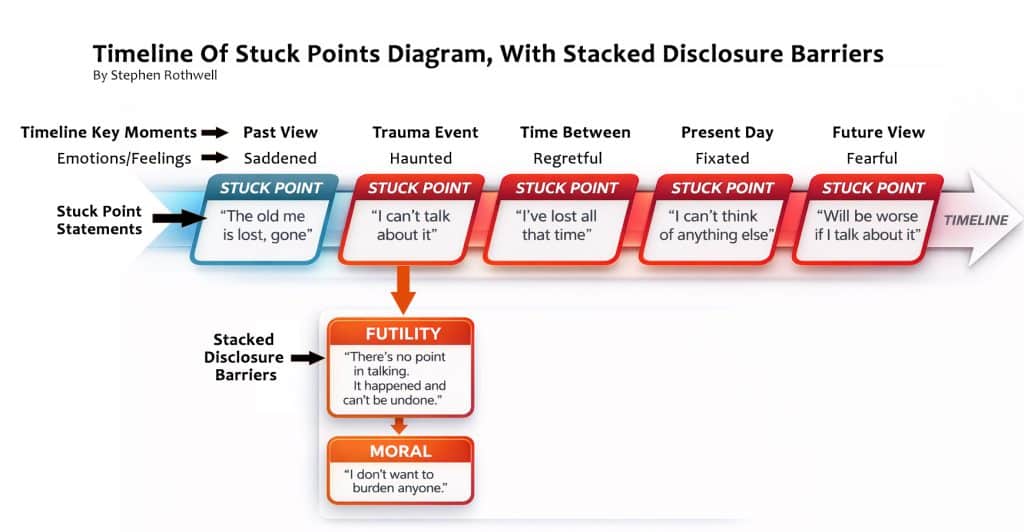
This is what we will call Stacked Disclosure Barriers.
A person might reveal:
- Disclosure Barrier 1: “There’s no point talking about it.” (Futility)
- Disclosure Barrier 2: “I don’t want to burden anyone.” (Moral)
This creates a closed system:
- It won’t help
- It’s not safe
No action feels possible.
No action feels justified.
Until each position is understood, the system holds.
Please see below for a diagram: Timeline of Stuck Points with Stacked Disclosure Barriers.
Where to From Here?
At this point, the therapist has something extremely valuable.
The client has revealed not just their distress, but the logic that sustains it.
This is where the work becomes precise:
- Futility blocks everything downstream
- Moral beliefs can mask deeper positions
Therapists tend to work with the barrier that makes all other work feel pointless or unsafe.
For the purposes of this article, we will begin with the disclosure barrier of futility.
Example 1: Futility Thinking – “There’s No Point”
“There’s no point talking about it. What happened can’t be undone.”
At first glance, this seems reasonable. And in one sense, it is true.
But beneath this statement sit deeper beliefs:
- “I am uniquely broken.”
- “My suffering is irredeemable.”
- “Nothing can change how I feel.”
From this position, not talking is logical.
The Unifying Principle of Futility Thinking
People do not open up simply because they feel understood.
They open up when they believe something useful can happen.
The barrier is often not:
“This hurts too much”
It is:
“This won’t help”
Understanding Futility Thinking
Futility thinking sounds rational:
- “Talking won’t change anything.”
- “Nothing will fix this.”
But the mind has shifted from:
“It won’t undo the past”
to
“Nothing can change how I experience it now”
That is the critical shift.
Why This Thinking Exists
Futility protects:
- You don’t have to try
- You don’t risk disappointment
- You don’t re-enter the pain
But it assumes the only purpose of talking is to fix the past.
What Therapy Actually Does
Therapy does not change what happened.
It changes what happens next.
It changes:
- How the experience is held
- How it is interpreted
- How it moves through you
A gap begins to form between:
- The painful event
- The belief it can never ease
A skilled therapist will explain and demonstrate that the (1) The painful event and (2) The belief that the hurt can never be reduced, are two different things.
From here:
- Rumination loosens
- Memories move toward acceptance
- The “negative future mirror” begins to weaken (the belief that the future will be as bad as or worse than today.)
The hurtful event still happened, and the memory of it will always be there, but the strongly felt relationship with the trauma can begin to ease, by degrees, until the previously all-consuming pain can be viewed through a lens of greater emotional comfort, and distance.
Eventually it becomes possible to walk alongside the memories, contextualising them as events that happened, but which do not have to interrupt one’s sense of journeying through life in pursuit of personally valuable goals.
Example 2: Moral Barrier – “I Don’t Want to Burden Anyone”
“I don’t want to put this on anyone.”
This is often strength, misapplied.
People are trying to:
- Protect others
- Avoid harm
- Carry their own weight
But the belief shifts from:
“I don’t want to harm others”
to
“My pain harms others”
When Silence Feels Right
From the outside, it looks like avoidance.
From the inside, it feels like integrity.
“I don’t want to put this onto other people.”
This aligns with values:
- I protect others
- I don’t hurt people
- I carry my own weight
Silence becomes loyalty to those values.
Why This Is Hard to Shift
When a belief attaches to identity, it feels like truth.
Therapy then looks like harm transfer.
Speaking feels like:
- Burdening
- Contaminating
- Imposing
So silence feels right.
The Hidden Assumption
“If I speak, others will feel what I felt.”
Trauma makes this feel true.
But therapy works differently.
A therapist:
- Contains
- Regulates
- Structures
They are not harmed by the material.
Why It Still Feels Unsafe
Many people have learned:
- Disclosure leads to dismissal
- Or overwhelm
So the nervous system says: “Be careful.”
Safety builds through experience, not reassurance.
Often the first step is the articulation of the disclosure barrier:
“I feel like if I talk about this, I’ll hurt you.”
Then:
- The belief becomes visible, and can be discussed
- The therapist invites small ‘test’ disclosures (sometimes framing them as ‘5%’ disclosures)
- The feared outcome does not occur
This begins to loosen the equation:
“If I speak, I cause harm.”
Final Position
“I can’t talk about it” is not a wall. It is a doorway.
Not into the trauma itself, not yet. But into the system of beliefs around it.
Once that system is:
- Visible
- Organised
- Understood
It can be worked with.
It can be questioned.
It can begin to loosen.
That is where movement starts.
Not all at once. Not completely.
But enough.
And often, enough is where everything begins.
Courtesy of www.reliefandhope.com
Important Caveat:
Some “I can’t talk about it” is not belief-driven. It is state-dependent:
- Freeze
- Shutdown
- Dissociation
Not all barriers are cognitive. Some are physiological constraints.
Evidence-Based Citations:
1. “I can’t talk about it” as information, not resistance
Principle: Client avoidance or silence contains clinically meaningful data rather than being obstruction.
- Judith Herman (1992). Trauma and Recovery.
→ Establishes that avoidance and silence are core trauma responses and meaningful indicators of psychological state. - Bessel van der Kolk (2014). The Body Keeps the Score.
→ Describes how trauma is encoded non-verbally and why clients may be unable, not unwilling, to speak. - Edna Foa & Kozak, M. (1986). Emotional processing of fear. Psychological Bulletin.
→ Avoidance is part of the fear structure and signals where therapeutic work is needed.
2. “Stuck points” as structured beliefs
Principle: Trauma-related beliefs are organised, not random, and maintain distress.
- Patricia Resick et al. (2017). Cognitive Processing Therapy for PTSD.
→ Defines “stuck points” as rigid maladaptive beliefs that maintain PTSD. - Resick, P. A., & Schnicke, M. K. (1992). Cognitive processing therapy. Journal of Consulting and Clinical Psychology.
→ Introduces the structured nature of trauma-related cognitions. - Aaron Beck (1976). Cognitive Therapy and the Emotional Disorders.
→ Foundational work on cognitive schemas shaping emotional responses.
3. Indirect processing (“talking about why you can’t talk”)
Principle: Approaching trauma indirectly is still therapeutic work.
- Marylene Cloitre et al. (2012). STAIR model.
→ Emphasises phased treatment and indirect engagement before trauma processing. - Herman (1992)
→ Phase-oriented trauma therapy: safety → remembrance → reconnection. - Pierre Janet (1907/modern interpretations)
→ Early work on dissociation and the need for gradual integration.
4. Mapping beliefs across time (timeline work)
Principle: Trauma impacts past, present, and future meaning-making.
- Janoff-Bulman (1992). Shattered Assumptions.
→ Trauma disrupts core beliefs about self, world, and future. - Ehlers & Clark, D. (2000). Cognitive model of PTSD. Behaviour Research and Therapy.
→ Persistent threat arises from maladaptive appraisals over time. - Donald Meichenbaum (1994). A Clinical Handbook.
→ Emphasises narrative reconstruction and meaning across timelines.
5. Making implicit systems visible
Principle: Naming and organising internal experiences reduces distress.
- Daniel Siegel (2010). Mindsight.
→ “Name it to tame it” concept, linking awareness to regulation. - James Pennebaker (1997). Expressive writing research.
→ Structuring emotional experience improves psychological outcomes. - Karl Weick (1995). Sensemaking in Organizations.
→ Coherence reduces chaos and improves functioning.
6. Belief loosening through cognitive reappraisal
Principle: Small shifts in rigid beliefs create therapeutic movement.
- Beck (1976)
→ Cognitive restructuring as core mechanism of change. - David Clark & Beck, A. (2010). Cognitive Therapy of Anxiety Disorders.
→ Examining beliefs reduces emotional intensity. - Ehlers & Clark (2000)
→ Updating trauma appraisals reduces PTSD symptoms.
7. “Stacked” or interacting barriers
Principle: Multiple beliefs interact to maintain avoidance.
- Steven Hayes et al. (1999). Acceptance and Commitment Therapy.
→ Cognitive fusion and experiential avoidance as interacting systems. - Marsha Linehan (1993). CBT for Borderline Personality Disorder.
→ Multiple reinforcing belief systems maintain behavioural patterns. - Paul Salkovskis (1996).
→ Safety behaviours and beliefs form self-reinforcing loops.
8. Futility thinking (“this won’t help”)
Principle: Engagement depends on perceived utility, not just distress tolerance.
- Albert Bandura (1977). Self-efficacy theory.
→ Behaviour depends on belief that action will produce results. - Irvin Yalom (2002). The Gift of Therapy.
→ Hope and perceived usefulness are central to engagement. - Frank & Frank (1991). Persuasion and Healing.
→ Therapy works partly by restoring expectation of benefit.
9. Therapy changes relationship to the past, not the past itself
Principle: Distress reduction comes from reprocessing, not erasing events.
- Edna Foa et al. (2007). Prolonged Exposure Therapy.
→ Emotional processing reduces distress without changing the event. - van der Kolk (2014)
→ Trauma memory integration changes lived experience. - Francine Shapiro (2001). EMDR.
→ Reprocessing alters emotional intensity and meaning.
10. Moral barriers and identity-linked beliefs
Principle: Values can reinforce avoidance when misapplied.
- Kristin Neff (2003). Self-compassion research.
→ Harsh self-standards often mask as morality. - Hayes et al. (1999)
→ Values can both guide and rigidify behaviour. - Brene Brown (2012). Daring Greatly.
→ Shame and fear of burdening others inhibit disclosure.
11. Gradual exposure and “test disclosures”
Principle: Safety is built through experience, not reassurance.
- Foa et al. (2007)
→ Gradual exposure reduces fear response. - Joseph Wolpe (1958). Systematic desensitisation.
→ Incremental exposure reduces anxiety. - Cloitre et al. (2012)
→ Skills + gradual disclosure improves outcomes.
12. Final principle: “The system becomes workable once visible”
Principle: Insight plus structure enables change.
- Siegel (2010)
- Pennebaker (1997)
- Ehlers & Clark (2000)
All converge on the same mechanism:
awareness → organisation → reappraisal → reduced distress
Photo Credit: Unsplash
Guest Post Disclaimer: This guest post is for educational and informational purposes only. Nothing shared here, across CPTSDfoundation.org, any CPTSD Foundation website, our associated communities, or our Social Media accounts, is intended to substitute for or supersede the professional advice and direction of your medical or mental health providers. The thoughts and opinions expressed are those of the guest author and do not necessarily reflect the views of the CPTSD Foundation. For further details, please review the following: Terms of Service, Privacy Policy and Full Disclaimer
- About the Author
- Latest Posts



